See also Getting to Grips with the Brain for a developmentally-based approach to the anatomy of these regions.
Something that is seen more frequently than actual laughter or tears is euphoria. Some patients may report that they feel "high", as if they have taken alcohol or other mood-altering drugs. This, again, is often attributed to release of endogenous opioids, but the same comments apply. Marked euphoria is not particularly common, but minor versions of it, generally described as a sense of calm or relaxation, occur in probably 30 or 40 per cent of cases.
Another effect, which is fortunately much less common than those I've just described, is an epileptic fit. These generally happen in patients who are not known to be epileptic. When they occur in patients who were sitting at the time they are usually attributed to vasovagal syncope causing temporary cerebral anoxia, but this may not be the whole story since they can also occur in patients who are lying down.
It is well known that patients who are unwilling to have acupuncture or are afraid of it seldom respond well to treatment; this has been noted in the traditional literature for many centuries. (On the other hand, belief in the efficacy of the treatment is unimportant).
All these things must, presumably, have a neurological explanation. They point to the occurrence of events in the central nervous system that have an effect on mood and behaviour, and what I should like to do is to think about some of the brain structures that may be involved.
Much of the current theorising about acupuncture concentrates on the spinal cord and brain stem, with particular reference to pain(2). However, this does not tell us much about the subjective phenomema of euphoria and so forth, so I think it is also the higher levels that we ought to be looking at, particularly the limbic system.
There is a widespread idea that this is a part of the brain that is closely concerned with emotion, so it might reasonably be thought to have something to do with unexplained laughter and tears, as well as with fear and euphoria. Actually, the idea that the limbic system is concerned with emotion is at best a half-truth, but there certainly is a connection, which is probably relevant to acupuncture. But before getting down to this we need to establish exactly what it is we're talking about here, because the limbic system is a rather slippery concept.
Anatomically, the main structures we have to consider become visible only when we split the brain sagitally into two halves and look at the inner or medial surface (3).
The limbic system is made up of the limbic lobe and certain additional structures.
The limbic lobe is on the inner aspect of the cortex, It partially surrounds the corpus callosum and is made up of the cingulate (which means belt-like) gyrus and the parahippocampal gyrus. These are connected to each other by a narrow isthmus beneath the splenium (posterior part) of the corpus callosum. The hippocampus, which is in the floor of the temporal horn of the lateral ventricle, is also included in the limbic lobe.
"Limbic" means "rim", as in the rim of a tennis racquet. One might wonder how the limbic lobe got that name, because in the human brain it is not all that conspicuous owing to the huge development of the cortex, but in other mammals, for example the rabbit, it forms a considerable part of the medial aspect of the hemisphere and really is a kind of rim, as the name implies. This was why Paul Broca coined the term in the 19th century. It was an anatomical, not a functional, description. Later this part of the brain was thought to be concerned with smell and was therefore called the rhinencephalon (meaning "nose brain").
The limbic system incorporates several additional structures:
To understand how this works, we need to take account of embryology and also the evolutionary history of the brain (4). What happens during its development is that the free margin of the developing brain (the pallium) becomes rolled upwards and then inwards to form the hippocampus. The part that is still at the surface, so to speak, is the parahippocampal gyrus. This folding process continues, now in the opposite direction, taking the free margin of the developing hippocampus outwards again, towards the medial surface of the temporal lobe. In this way the free margin of the hippocampus becomes doubled out and forms the dentate gyrus, which is separated from the parahippocampal gyrus by the hippocampal sulcus. ("Dentate" refers to the fact that its margin is serrated.) As a result of this repeated folding the mature hippocampus comes to consist of two interlocking sections of tubes. In cross-section it looks rather like a swiss roll. Hence we can speak of the hippocampal formation, consisting of the hippocampus, the dentate gyrus, and most of the parahippocampal gyrus.
The name hippocampus means seahorse, but I think myself that it more closely resembles a scorpion without legs. The head of the scorpion lies close to the amygdala at the tip of the temporal lobe and the body extends posteriorly, ending below the splenium of the corpus callosum. The tail of the scorpion is represented by a band of efferent and afferent fibres which form a ridge along its medial border called the fimbria. The left and right fimbriae continue as the crura of the fornix, which run from the hippocampus backwards, upwards, and then forwards beneath the corpus callosum. The "tails" of the two hippocampuses, i.e the two fimbriae, join up for a time to form the body of the fornix before separating again to descend as the columns of the fornix and finally reach the mammillary bodies of the hypothalamus on each side.
Histologically, the parahippocampal gyrus is 6-layered or almost so (i.e. neocortex) but the hippocampus is 3-layered (archicortex); there is a transition in structure at the "bend" called the subiculum. The pyramidal cell layer of the hippocampus is continuous with layer 5 (internal pyramidal) of the cortex. Certain of the hippocampal cells are thought to show an effect called longterm potentiation (LTP), which lasts for several days and is believed to be involved in the formation of new memories.
The hippocampus varies in size in different animals and reaches its largest absolute and relative size in humans. This suggests that it has some important role in human consciousness.
To understand this, we have to see how the limbic system idea has developed (4).
Common sense says that, when you see a bear in the wood (James's example), you feel frightened: your stomach churns, you start to sweat, and you run away. This implies that the emotion of fear causes the physical effects. James however said that, when you see the bear, this directly causes the physical effects of sweating, churning stomach, and running away, and it is the awareness of these physical events that constitutes the feeling of fear. In other words, in James's view the emotion is caused by the physiological changes, not the other way about.
In the 1920s Walter Cannon and Philip Bard put forward a somewhat similar theory. They suggested that seeing the bear causes changes in the thalamus; these in turn are transmitted to the hypothalamus and thence to the muscles and organs, and it's the events in your brain that are perceived as fear. (This is the famous "fright and flight" reaction.) In other words, they moved the centre of interest from the periphery to the brain, and especially the hypothalamus.
Cannon disagreed with James's idea but in fact his own theory isn't all that different; it just focuses on different physiological phenomena.
There was however apparently a difficulty with this theory: the cortex was thought not to be directly connected to the hypothalamus, so how could changes in the hypothalamus reach consciousness?
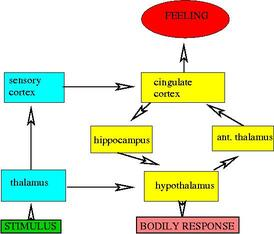
Then in 1937 James Papez put forward a new theory which was destined to become very influential. He went back to Broca's notion and suggested that the limbic lobe was responsible for emotion. Information was supposed to flow in a circuit from the hypothalamus to the medial cortex and back again.
The sequence is as follows: parahippocampal gyrus (entorhinal area) - hippocampus - mammilary bodies (hypothalamus) - thalamus (anterior nuclei) - cingulate gyrus - parahippocampal gyrus. This is the famous Papez circuit.
In it, the cingulate gyrus has a central role; it is supposed to be "emotional cortex" and analogous to the sensory cortex in the parietal lobe. The hippocampus is also concerned with emotion. This was a mistake, but nevertheless the theory was a brilliant anticipation of later anatomical discoveries.
Paul MacLean took up the Papez theory in 1949 and elaborated it. He suggested that the hippocampus was what he called an "emotional keyboard" (a bit like the Organ of Corti?). He continued to elaborate this idea as the years went by and in 1970 he introduced the notion of the "triune brain", made up as follows:
On the merit side, it sets emotion in an evolutionary context, and it may explain some of the psychiatric symptoms (dissociation of intellect and emotion) that MacLean claimed it did. But the distinction between "old" and "new" cortex is no longer accepted (for this reason, some authorities now prefer to avoid terms like "neocortex" and "archicortex" and speak of "isocortex" and "allocortex" instead). It also appears that the forebrain is actually phylogenetically older than the midbrain and hindbrain (14). Moreover, damage to the hippocampus and mamillary bodies has little effect on emotion but a great deal of effect on memory, contrary to what MacLean predicted.
So why has the theory survived so long? Partly because it is a convenient shorthand to name the areas between the hypothalamus and "neocortex", and partly because these structures, especially the amygdala, do have something to do with emotion; the theory is not completely wrong. But to call the limbic system the emotional centre of the brain is certainly misleading (5,6).
I'll give just one example (7). In a recent study, healthy volunteers were given tactile stimulation to the right side of the lower lip for a few minutes. Then they were given painful electrical stimulation to the median nerve on the same side. When the lip stimulation was repeated, some of them felt this both at the lip and at the site in the wrist where the painful stimulus had been applied; one of these subjects actually felt that her fist was clenched. This of course is something that patients with phantom limbs sometimes report. So this study suggests that even brief peripheral painful stimulation can temporarily alter sensory cortical mapping. I therefore find it quite plausible to suppose that it can also modulate activity in the anterior cingulate cortex and other limbic system structures.
Professor Thompson and his colleagues (8) have found that patients differ considerably in their responses to transcutaneous electrical nerve stimulation (TENS). Individual patients tend to have preferred frequency of stimulation and pattern of stimulation, which is constant for those individuals, so these authors suggest that lack of response to TENS may be linked to low central nervous system responsiveness to sensory stimuli in general. It seems plausible that the same is true of acupuncture sensitivity. Strong reactors would then be people whose central nervous system, including the limbic system, is particularly sensitive to sensory stimulation. In the case of the limbic system there are nociceptive receptors in the cingulate cortex that have large receptive fields that may encompass the whole body (9). Strong reactors may therefore be people with many such receptors.
What all this suggest is that strong reactors may be people in whom these structures are more easily influenced by sensory stimulation, either to depress the amygdala or to stimulate the anterior cingulate.
I have been treating a relative for Liver Wind (manifesting as one tonic-clonic seizure followed by periods of intense dizziness, which have ceased during six weeks or so of conventional medication and regular acupuncture/moxa). I believe the Liver Wind stems from long term Liver Qi Stagnation and also Liver Blood deficiency.My correspondent says that her relative enjoyed the out-of-body experience so much that he was reluctant to mention it in case she stopped the treatment! The neurologist confirmed that the "dizziness" episodes were minor absences; they have ceased after the patient started taking carbamazepine.In the last four treatments I have used LI4 and LR3, plus sometimes SP6, and always moxa on KI1. He dislikes needles (but suffers them!), but has always reported great effect from the moxa, such as feeling a sensation connect his feet to his head, and says it makes him very relaxed. He has also reported feeling what I would call more grounded between treatments - he says when he is walking he feels he is more in his hip area than his head.
In the last treatment (as above, no SP6) he reported, towards the end of the moxa session, feeling like he had left his body, and been floating. He had felt himself turn around until his feet were nearly by the head of his body, and then back, and then rotate to his left so he was on his left side, and then back again. I stopped treatment, and he said he was back where he should be and feeling great.
A report has recently appeared describing out-of-body experiences produced by brain stimulation at the right anglular gyrus in a patient who was undergoing evaluation for epilepsy treatment (1). The patient had right temporal-lobe epilepsy. The authors suggest that the experience of dissociation of self from the body is a result of failure to integrate complex somatosensory and vestibular information.
All the structures we have been considering are frequently implicated in epilepsy, especially epilepsy with strange subjective phenomena not necessarily accompanied by loss of consciousness. This is called complex partial epilepsy, or temporal lobe epilepsy. Temporal lobe epilepsy can cause difficulties in speaking, and I've noticed that some strong reactors also seem to find a certain degree of this while being needled.
There are similarities between temporal lobe epilepsy and some kinds of migraine aura, and the fact that acupuncture seems to help some patients who suffer from migraine with aura may be connected with this. Moreover, the authors of the procaine study I cited just now say that patients with anxiety disorders report an increased incidence of spontaneous paroxysmal and emotional phenomena similar to those of patients with complex partial epilepsy, which may be due to limbic dysfunction (10).
Arroyo and colleagues have described three patients with seizures who shed light on this question (12). In one, the onset of seizures was in the left anterior cingulate region. This patient didn't feel amused although she was laughing. The other two didn't laugh during seizures but laughter was elicited by electrical stimulation of the parahippocampal gyrus and neighbouring cortex, and both of these actually felt amused during stimulated laughter.
These observations suggest that laughter can be produced by activation of parts of the limbic system, though there differences according to the exact site of stimulation.
However, there is also another possibility, based on a suggestion by Ramachandran (13).
Patients with a condition called pain asymbolia feel pain but don't experience the emotional accompaniment. Moreover, some patients with this disorder giggle when pricked. This, of course, is exactly what happens in acupuncture. So it's tempting to see a clue to why acupuncture causes laughter here, but there is a problem: pain asymbolia is pathological; it may be due to damage to the insular cortex, which receives pain input and projects to the anterior cingulate cortex, whereas acupuncture-related laughter usually occurs in the presence of an intact nervous system. We might suppose that acupuncture can temporarily disconnect the insular cortex from the anterior cingulate, to produce a kind of temporary "pain asymbolia".
There is, however, also another idea, again based on a hypothesis put forward by Ramachandran about the reason we laugh when we are tickled. He thinks that laughter generally occurs when we perceive an incongruity; this is the basis of many jokes and also the reason we may laugh when a pompous man slips on a banana skin. Ramachandran suggests that they perceive an incongruity between an apparent physical threat and a context of play; this makes them laugh. This theory explains why one can't easily tickle oneself; one knows in advance that there is no threat involved.
Now, acupuncture is also a kind of physical threat, in that (relatively minor) pain is inflicted but in a therapeutic context. Also, one may expect the needle to be painful and then be pleasantly surprised when it's not as bad as expected. There may thus be a functional dissociation between the insula and the anterior cingulate cortex. The insular cortex registers the needle prick as a threat but the cingulate cortex doesn't agree, hence there is a perceived incongruity resulting in laughter. On this hypothesis, acupuncture is a kind of tickling.
In the meantime, I find that if one reflects on what is known about this very complex system it does shed light on some of the more curious phenomena which we encounter from time to time while needling our patients.